Wednesday, January 26, 2011
PULMONARY ARTERY PRESSURE MONITORING
PULMONARY ARTERY PRESSURE MONITORING
Pulmonary artery pressure monitoring is measuring the pressure in the pulmonary artery leading to the lungs. It also allows for indirect measurement of left heart pressures since the pulmonary veins have no valves in them and collects the information needed to calculate cardiac output and resistance. The PA catheter assesses all 3 components of stroke volume: preload, afterload, and contractility.
The catheter is 60-100 cm long and the caliber is 4-8 Fr (a standard suction catheter is 14 French)...the balloon will hold 0.5-1.5 ml of air and get 8-13 mm big when inflated
Distal Port:
• terminates in the pulmonary artery
• used to monitor pulmonary artery pressure and pulmonary capillary wedge pressure when the balloon is inflated
• provides a port for mixed venous blood samples
Balloon Inflation Port:
• used to inflate the balloon at the end of the PA catheter with no more than 1.5 ml of air
• has a locking device for safety
• is inflated during insertion to allow the catheter to float into correct position
• when inflated will measure pulmonary capillary wedge pressure, which is equal to the pressure in the left atrium and ventricle during diastole
Proximal Injectate Port:
• is usually blue in color
• provides a port for injecting fluid when measuring CO
• measures RA/CVP
• can be used as an IV infusion site if CVP monitoring not needed
Proximal Infusion Port:
• is usually white in color and AKA venous infusion port
• lumen opens into the RA
• can be used to infuse fluids or meds without interruption
• is not attached to the transducer
Cardiac Output Port:
• a white square port with pins that connects to the CO cable
• the CO cable connects to the monitor
• has temperature sensitive wires that terminate near the distal tip
• Pace Port for a ventricular or atrial pacemaker
• SvO2 monitoring port
Pulmonary artery pressure monitoring is measuring the pressure in the pulmonary artery leading to the lungs. It also allows for indirect measurement of left heart pressures since the pulmonary veins have no valves in them and collects the information needed to calculate cardiac output and resistance. The PA catheter assesses all 3 components of stroke volume: preload, afterload, and contractility.
The catheter is 60-100 cm long and the caliber is 4-8 Fr (a standard suction catheter is 14 French)...the balloon will hold 0.5-1.5 ml of air and get 8-13 mm big when inflated
Distal Port:
• terminates in the pulmonary artery
• used to monitor pulmonary artery pressure and pulmonary capillary wedge pressure when the balloon is inflated
• provides a port for mixed venous blood samples
Balloon Inflation Port:
• used to inflate the balloon at the end of the PA catheter with no more than 1.5 ml of air
• has a locking device for safety
• is inflated during insertion to allow the catheter to float into correct position
• when inflated will measure pulmonary capillary wedge pressure, which is equal to the pressure in the left atrium and ventricle during diastole
Proximal Injectate Port:
• is usually blue in color
• provides a port for injecting fluid when measuring CO
• measures RA/CVP
• can be used as an IV infusion site if CVP monitoring not needed
Proximal Infusion Port:
• is usually white in color and AKA venous infusion port
• lumen opens into the RA
• can be used to infuse fluids or meds without interruption
• is not attached to the transducer
Cardiac Output Port:
• a white square port with pins that connects to the CO cable
• the CO cable connects to the monitor
• has temperature sensitive wires that terminate near the distal tip
• is used for thermodilution CO measurement
Other Ports:• Pace Port for a ventricular or atrial pacemaker
• SvO2 monitoring port
Tuesday, January 25, 2011
THE ROLE OF 10, Mitral reguregitation

These are 10 points you can remember about a particular subjects.Tthese 10 points if you speak about during your viva session your examiner will be thrilled.
If you expand each point during written exam you can cover the subject effeciently.
If you apply them clinically you patient is saved.
- Acute MRis ususlly due to myocardia ischemia, infective endocarditis, or chest trauma.
- Chronic MR is due to rheumatic fever, congenital abnormality in valve apparatus.
- The principal derangement is reduction inforward stroke volume causing symptoms of low cardiac output.
- Chronic MR usually presents as low COP symptoms because left atrium has time to dilate and accomodate the reguritanat blood.
- Acute MR presents as pulmonary congestion or hypertension, because aleft atrium dose not have time to dilate to accomodate the reguritant blood.
- Anesthetic goals: avoid bradycardia, increase in afterload( both will increase the regurgitant volume), hear rate should ideally kept between 80-100/m.
- Premedication may decrease stress elevation of afterload but shoyld be used cautiously as co2 elevation may increase pulmonary pressure in patient with pulmonary hypertension.
- Spinal and epidural cen be tolerated in patients with preserved ventricular function.
- Opioid based technique is preferrable to inhalational agents in patients with moderate to severe ventricular impairment.
- Pancuronium can be useful slection of muscle relaxant agents in combination with opioids.
Monday, January 24, 2011
Aortic stenosis, role of 10
What is the role of 10?
These are 10 points you can remember about a particular subjects.Tthese 10 points if you speak about during your viva session your examiner will be thrilled.
If you expand each point during written exam you can cover the subject effeciently.
If you apply them clinically you patient is saved.
Aortic stenosis(AS)
Aortic-LV pressure gradient 16-34mmHg 35-75 ˃ 75
4. Anesthetic goals:
6. Spinal and epidural are contraindicated in patients with severe AS.
7. Induction: primarily opioid based or combination of ketamine and benzodiazepine.
8. Maintenance is with opioid based technique.
9. Vecuronium, rocuronium can be used as muscle relaxant. Pancuronium is best avoided.
10. Phenylephrine is preferred as vasopressor over ephedrine because it lacks B agonist activity.
These are 10 points you can remember about a particular subjects.Tthese 10 points if you speak about during your viva session your examiner will be thrilled.
If you expand each point during written exam you can cover the subject effeciently.
If you apply them clinically you patient is saved.
Aortic stenosis(AS)
- It is nearly always congenital, rheumatic or degenerative
- AS---LV hypertrophy, reduced LV compliance, diastolic dysfunction.LV filling is quiet dependant on normal atrial contraction.
- Graded into: Mild Moderate severe
Aortic-LV pressure gradient 16-34mmHg 35-75 ˃ 75
4. Anesthetic goals:
- maintain sinus rhythm
- Maintain heart rate 60-90/m
- Maintain intravascular volume.
6. Spinal and epidural are contraindicated in patients with severe AS.
7. Induction: primarily opioid based or combination of ketamine and benzodiazepine.
8. Maintenance is with opioid based technique.
9. Vecuronium, rocuronium can be used as muscle relaxant. Pancuronium is best avoided.
10. Phenylephrine is preferred as vasopressor over ephedrine because it lacks B agonist activity.
Mitral stenosis, role of 10
What is the role of 10?
These are 10 points you can remember about a particular subjects.
These 10 points if you speak about during your viva session your examiner will be thrilled.
If you expand each point during written exam you can cover the subject effeciently.
If you apply them clinically you patient is saved.
Mitral stenosis(MS)
1. MS is almost always caused by rheumatic fever, commonly in conjunction with other valvular lesions
2. MS---left atrial volume and pressure overload----LA dilataion----increased PVR---pulmonary hypertension----right ventricular hypertrophy and failure.
LA dilatation--- promotes AF and embolic events.
3. Graded into
Mild Moderate severe
MITRAL VALVE AREA 2-1.5 cm 2 1.6-1 ˂1
Lv-LA pressure gradient 2-6 mmHg 6-12 ˃ 12
Pressure half time 100ms 200 300
4. Anesthetic goals
6. Induction is with standard IV agents with possible exception of ketamine
7. Maintainance is with opioid based technique
8. N2O may increase PVR and cause pulmonary hypertension
9. Vecuronium, rocuronium can be used as muscle relaxant. Pancuronium is best avoided.
10. Phenylephrine is preferred as vasopressor over ephedrine because it lacks B agonist aactivity.
These are 10 points you can remember about a particular subjects.
These 10 points if you speak about during your viva session your examiner will be thrilled.
If you expand each point during written exam you can cover the subject effeciently.
If you apply them clinically you patient is saved.
Mitral stenosis(MS)
1. MS is almost always caused by rheumatic fever, commonly in conjunction with other valvular lesions
2. MS---left atrial volume and pressure overload----LA dilataion----increased PVR---pulmonary hypertension----right ventricular hypertrophy and failure.
LA dilatation--- promotes AF and embolic events.
3. Graded into
Mild Moderate severe
MITRAL VALVE AREA 2-1.5 cm 2 1.6-1 ˂1
Lv-LA pressure gradient 2-6 mmHg 6-12 ˃ 12
Pressure half time 100ms 200 300
4. Anesthetic goals
- maintain sinus rhytm
- Avoid tachycardia
- Avoid hypovolemia, hypervolemia
6. Induction is with standard IV agents with possible exception of ketamine
7. Maintainance is with opioid based technique
8. N2O may increase PVR and cause pulmonary hypertension
9. Vecuronium, rocuronium can be used as muscle relaxant. Pancuronium is best avoided.
10. Phenylephrine is preferred as vasopressor over ephedrine because it lacks B agonist aactivity.
Sunday, January 23, 2011
put a smile on your face

"I love you too," I said, with a dopey grin plastered on my face. I was about to hang up when I heard him ask sweetly, "Mommy, who was that?"
Saturday, January 22, 2011
THE ROLE OF 10
what is the role of 10?
these are 10 points you can remember about a particular subjects.
these 10 points if you speak about during your viva session your examiner will be thrilled.
if you expand each point during written exam you can cover the subject effeciently.
if you apply them clinically you patient is saved.
Tetralogy of Fallot
these are 10 points you can remember about a particular subjects.
these 10 points if you speak about during your viva session your examiner will be thrilled.
if you expand each point during written exam you can cover the subject effeciently.
if you apply them clinically you patient is saved.
Tetralogy of Fallot
- the most common cyanotic heart disease in adult populations.
- it includes: right ventricular outflow obstruction, right ventricular hypertrophy, VSD, and oerriding aorta.
- pathophysiolgy: reduced pulmonary blood flow causing arterial hypoxemia and cyanosis and there is R-L shunt through VSD.
- cyanotic spell: infundibular spasm or constriction causing reduction of pulmonary blood flow and increase in right ventricular pressure leading to increase of R-L shunt. (do not forget its management).
- pink tet: refers to any noncyanotic patient with fallot with increased pulmonary blood flow due to large PDA or major Aortopulmonary arterial colateral.
- palliative shunts: waterson, Apotts, central. blalock Taussig.
- anesthetic goals: maintain intravascular volume, maintain SVR, avoid increase in PVR.
- IM induction with katamine, glycopyrolate, succinyl choline.
- maintainance: nitrous oxide + ketamine, pancuronium, mechanical ventilation with low airway pressure.
- intraoperative monitoring: the difference between PaCO2 and ETCO2 will increase if intraoperative R-L shunt increase as in tet spell.
Friday, January 21, 2011
Thursday, January 20, 2011
Tuesday, January 18, 2011
pediatric nerve blocks
•Introduction
•Equipment
•Local Anesthetics
•Nerve Localization Methods
•Head & Neck Blocks
•Upper Extremity Blocks
•Nerve Block At The Wrist
•Lower Extremity Blockade
•Trunk Blocks
•Summary
IntroductionThe use of peripheral nerve blocks has been regaining significant popularity in the daily practice of most anesthesiologists. Despite the trend towards increase in the use of regional anesthesia and nerve blocks in adults, peripheral nerve blocks in children remain underutilized. Common reasons include the concern of neurologic complications and the lack of technical skills required for successful use of peripheral nerve blocks. Although performance of PNBs in anesthetized adults is often debated, such practice is well accepted in pediatric patients. A large prospective database collected in France demonstrated no increased incidence of complications when regional anesthesia, particularly when peripheral nerve blocks were performed under general anesthesia.1 The incidence of regional anesthesia related complications in one study was less than 0.9/1000 anesthetic procedures performed. When used with skill, the success and complications of performance of peripheral nerve blocks in children should not be significantly different from those in the adults. In addition, the equipment used for PNBs in children is similar to that used in adults (see Chapter 17). Although most peripheral nerve blocks are performed in an operating room environment, the use of regional anesthesia in children extends to an emergency department 2 as well as in an intensive care unit setting.3;4 The key to success of peripheral nerve blockade in children is the proper knowledge of the anatomy, pharmacology, equipment used for regional anesthesia and effective use of pre-procedure sedation and analgesia.
•Equipment
•Local Anesthetics
•Nerve Localization Methods
•Head & Neck Blocks
•Upper Extremity Blocks
•Nerve Block At The Wrist
•Lower Extremity Blockade
•Trunk Blocks
•Summary
IntroductionThe use of peripheral nerve blocks has been regaining significant popularity in the daily practice of most anesthesiologists. Despite the trend towards increase in the use of regional anesthesia and nerve blocks in adults, peripheral nerve blocks in children remain underutilized. Common reasons include the concern of neurologic complications and the lack of technical skills required for successful use of peripheral nerve blocks. Although performance of PNBs in anesthetized adults is often debated, such practice is well accepted in pediatric patients. A large prospective database collected in France demonstrated no increased incidence of complications when regional anesthesia, particularly when peripheral nerve blocks were performed under general anesthesia.1 The incidence of regional anesthesia related complications in one study was less than 0.9/1000 anesthetic procedures performed. When used with skill, the success and complications of performance of peripheral nerve blocks in children should not be significantly different from those in the adults. In addition, the equipment used for PNBs in children is similar to that used in adults (see Chapter 17). Although most peripheral nerve blocks are performed in an operating room environment, the use of regional anesthesia in children extends to an emergency department 2 as well as in an intensive care unit setting.3;4 The key to success of peripheral nerve blockade in children is the proper knowledge of the anatomy, pharmacology, equipment used for regional anesthesia and effective use of pre-procedure sedation and analgesia.
Monday, January 17, 2011
oh, the patient with jaundice. what can I do?
The jaundiced patient must be always taken seriously, and an accurate preoperative diagnosis of the cause is important. Three major category of diseases can cause jaundice:
an accurate daignosis of the type and cause of jaundice can be reached by taking a careful history, a review of liver function tests, and other investigations.
history:
history of family jaundice, contact with jaundice patient, blood transfusion, tattooing, acupuncture, drug addiction,foreign travel, alcoho; intake, general health, and occupational hazards.
investigations:
liver function tests
full blood count:
A low blood count may be the result of concealed blood loss or hemolysis.
A raised white blood count may be seen with cholicystitis or cholangitis.
urea and electrolytes:
rising urea is important and require uergent treatment.
clotting studies:
PT may be prolonged.
virology:
hepatitis B may need to be excluded.
radiograpgs:
chest; both cholecystitis and hepatomegaly inhibit right sided diaphragmatic movements, thus giving a propensity for lower right chest infections and pulmonary effusions.
abdominal; only in aminority of cases the radiograph shows gall stones (ground glass appearance).
barium meal or endoscopy: it will reveal esophageal varices. distorsion and fixation od doudenum occurs in carcinoma of pancreas.
cholangiography: ERCP has a low complication rate and is effective at demonstrating the site of obstruction,even when the obstruction is complete.
ultrasonography and CT
thes investigations will demonstrate grossly dilated ducts and will give information about liver parynchema, gall baldder, and even the site of obstruction.
liver biopsy:
percutaneous needle biopsy is now accepted as a routine investigation in liver diseases.
the perioperative management depends on reaching a correct diagnosis of the type and cause of jaundice.
- prehepatic( unconjugated hyperbilirubinemia)
- hemolytic anemias
- gilbert syndrome
- Crigler Najar syndrome
- hepatic parynchemal diseases, furthur divided into acute or chronic
- biliary obstruction(intrahepatic or extrahepatic)
an accurate daignosis of the type and cause of jaundice can be reached by taking a careful history, a review of liver function tests, and other investigations.
history:
history of family jaundice, contact with jaundice patient, blood transfusion, tattooing, acupuncture, drug addiction,foreign travel, alcoho; intake, general health, and occupational hazards.
investigations:
liver function tests
full blood count:
A low blood count may be the result of concealed blood loss or hemolysis.
A raised white blood count may be seen with cholicystitis or cholangitis.
urea and electrolytes:
rising urea is important and require uergent treatment.
clotting studies:
PT may be prolonged.
virology:
hepatitis B may need to be excluded.
radiograpgs:
chest; both cholecystitis and hepatomegaly inhibit right sided diaphragmatic movements, thus giving a propensity for lower right chest infections and pulmonary effusions.
abdominal; only in aminority of cases the radiograph shows gall stones (ground glass appearance).
barium meal or endoscopy: it will reveal esophageal varices. distorsion and fixation od doudenum occurs in carcinoma of pancreas.
cholangiography: ERCP has a low complication rate and is effective at demonstrating the site of obstruction,even when the obstruction is complete.
ultrasonography and CT
thes investigations will demonstrate grossly dilated ducts and will give information about liver parynchema, gall baldder, and even the site of obstruction.
liver biopsy:
percutaneous needle biopsy is now accepted as a routine investigation in liver diseases.
the perioperative management depends on reaching a correct diagnosis of the type and cause of jaundice.
Friday, January 14, 2011
what is the function of skin?!!!
A grade school teacher was grading a science test on the human body, The first question was, "Name one of the major functions of your skin."
One child had written: "To keep people who look at you from throwing up."
One child had written: "To keep people who look at you from throwing up."
Wednesday, January 12, 2011
Tuesday, January 11, 2011
Anesthesia in a patient with Gilbert's syndrome. Case report
 |
| nice example of Gilbert syndrome |
INTRODUCTION
Gilbert's syndrome is a chronic benign disease characterized by increased indirect bilirubin and clinically manifested as jaundice, which may appear before, during or after anesthesia.
Patients have jaundice when submitted to stress or exercises, during active menstrual cycle bleeding or when fasting 1. The incidence of this disease is estimated in 6% of general population 2, being more frequent in males 1-3.
Bilirubin is originated as from heme ring catabolism which may come from aged hemoglobins, bone marrow erythrocytes by ineffective erythropoiesis, or from blood proteins, especially liver blood proteins 3. After being uptaken by the reticuloendothelial system 3, heme-oxygenase breaks down hemoglobin in biliverdin, carbon monoxide and iron 4. Biliverdin-reductase converts biliverdin into bilirubin 4 at a rate of 4 mg/kg/day 3. This bilirubin is liposoluble and apolar. It may bind to albumin and its free fraction may cross blood-brain barrier 3. Bound to albumin, it is taken to the liver where it suffers conjugation with glycuronic acid becoming hydrosoluble and polar.
Jaundice is a clinical presentation characterized by yellowish skin, mucosa or eyes, when bilirubin is above 2.5 to 3 mg/dL 3.
Pregnant women or those under oral contraceptives develop less jaundice because in such conditions there is liver glucuronosyltransferase induction 2.
Syndrome may be diagnosed by family history, duration of the disease, lack of other liver diseases justifying jaundice, and jaundice triggered by predisposing factors, such as fasting, menstruation, stress and exercises 1. Diagnosis may be confirmed by jaundice improvement after fenobarbital and worsening after intravenous nicotinic acid 1.
This report aimed at presenting the case of Gilbert's syndrome patient submitted to general anesthesia for videolaparoscopic correction of gastroesophageal reflux.
Sunday, January 9, 2011
Anesthesia for liver cirrhosis
CIRRHOSIS
Cirrhosis is a serious and progressive disease that eventually results in hepatic failure.
causes include
• chronic active hepatitis (postnecrotic cirrhosis),
• chronic biliary inflammation or obstruction (primary biliary cirrhosis, sclerosing cholangitis),
• chronic right-sided congestive heart failure (cardiac cirrhosis),
• autoimmune hepatitis,
• hemochromatosis,
• Wilson's disease,
• 1-antitrypsin deficiency,
• nonalcoholic steatohepatitis, and
• cryptogenic cirrhosis.
Preoperative Considerations
Patients with cirrhosis are at increased risk for deterioration of liver function because of their limited functional reserves.
Successful anesthetic management of these patients is dependent on recognizing the multisystem nature of cirrhosis and controlling or preventing its complications
Gastrointestinal Manifestations
Portal hypertension (> 10 mm Hg) leads to the development of extensive portal-systemic venous collateral channels. Four major collateral sites are generally recognized: gastroesophageal, hemorrhoidal, periumbilical, and retroperitoneal.
In patients with cirrhosis, massive bleeding from gastroesophageal varices is a major cause of morbidity and mortality. In addition to the effects of acute blood loss, the increased nitrogen load (from the breakdown of blood in the intestinal tract) can precipitate hepatic encephalopathy.
The treatment of variceal bleeding is generally supportive (medical).
Blood loss should be replaced with intravenous fluids and blood products.
Nonsurgical treatment includes vasopressin (0.1–0.9 U/min intravenously), somatostatin (250 g followed by 250 g/h), propranolol, balloon tamponade (with a Sengstaken–Blakemore tube), and endoscopic sclerosis of the varices.
Percutaneous transjugular intrahepatic portosystemic shunts (TIPS) can reduce portal hypertension and subsequent bleeding (however, it may increase the incidence of encephalopathy).
When the bleeding fails to stop or it recurs, emergency surgery may be indicated. Surgical risk has been shown to correlate with the degree of hepatic impairment, based on clinical and laboratory findings. Shunting procedures are generally performed on low-risk patients, whereas ablative surgery, esophageal transection, and gastric devascularization are reserved for high-risk patients.
Child's Classification for Evaluating Hepatic Reserve.1
Risk Group A B C
Bilirubin (mg/dL) < 2.0 2.0–3.0 > 3.0
Serum albumin (g/dL) > 3.5 3.0–3.5 < 3.0
Ascites None Controlled Poorly controlled
Encephalopathy Absent Minimal Coma
Nutrition Excellent Good Poor
Mortality rate (%) 2–5 10 50
Hematological Manifestations
Anemia, thrombocytopenia, and, less commonly, leukopenia, may be present. The cause of the anemia is usually multifactorial and includes blood loss, increased red cell destruction, bone marrow suppression, and nutritional deficiencies.
Congestive splenomegaly (from portal hypertension) is largely responsible for the thrombocytopenia and leukopenia.
Coagulation factor deficiencies arise as a result of decreased hepatic synthesis. Enhanced fibrinolysis secondary to decreased clearance of activators of the fibrinolytic system may also contribute to the coagulopathy.
coagulopathy should be corrected before surgery. Clotting factors should be replaced with appropriate blood products such as FFP and cryoprecipitate.
Platelet transfusions should be considered immediately prior to surgery for counts less than 100,000/ L.
what you should remember about liver
HEPATIC PHYSIOLOGY & ANESTHESIA :
FUNCTIONAL ANATOMY
The liver is separated by the falciform ligament into right and left anatomic lobes; the larger right lobe has two additional smaller lobes at its posterior–inferior surface, the caudate and quadrate lobes. In contrast, surgical anatomy divides the liver based on its blood supply. Thus the right and left surgical lobes are defined by the point of bifurcation of the hepatic artery and portal vein (porta hepatis); the falciform ligament therefore divides the left surgical lobe into medial and lateral segments. Surgical anatomy defines a total of eight segments.
The liver is made up of 50,000–100,000 discrete anatomic units called lobules. Each lobule is composed of plates of hepatocytes arranged cylindrically around a centrilobular vein. Four to five portal tracts, composed of hepatic arterioles, portal venules, bile canaliculi, lymphatics, and nerves, surround each lobule.
In contrast to a lobule, an acinus, the functional unit of the liver, is defined by a portal tract in the middle and centrilobular veins at the periphery. Cells closest to the portal tract (zone 1) are well oxygenated; those closest to centrilobular veins (zone 3) receive the least oxygen and are most susceptible to injury.
FUNCTIONAL ANATOMY
The liver is separated by the falciform ligament into right and left anatomic lobes; the larger right lobe has two additional smaller lobes at its posterior–inferior surface, the caudate and quadrate lobes. In contrast, surgical anatomy divides the liver based on its blood supply. Thus the right and left surgical lobes are defined by the point of bifurcation of the hepatic artery and portal vein (porta hepatis); the falciform ligament therefore divides the left surgical lobe into medial and lateral segments. Surgical anatomy defines a total of eight segments.
The liver is made up of 50,000–100,000 discrete anatomic units called lobules. Each lobule is composed of plates of hepatocytes arranged cylindrically around a centrilobular vein. Four to five portal tracts, composed of hepatic arterioles, portal venules, bile canaliculi, lymphatics, and nerves, surround each lobule.
In contrast to a lobule, an acinus, the functional unit of the liver, is defined by a portal tract in the middle and centrilobular veins at the periphery. Cells closest to the portal tract (zone 1) are well oxygenated; those closest to centrilobular veins (zone 3) receive the least oxygen and are most susceptible to injury.
Saturday, January 8, 2011
Friday, January 7, 2011
just for laugh
A woman received a phone call that her daughter was very sick with a fever. She left work and stopped by the pharmacy for some medication for her daughter. When she returned to her car she was dismayed to find she had locked her keys inside. Somehow she had to get home to her sick daughter, but she didn't know what to do.
She called home to the baby sitter, who told her that her daughter was getting worse. However, the baby sitter did offer some advice.
"If you could find a coat hanger you may be able to use that to open the door."
The woman obtained an old rusty coat hanger from the pharmacy, but when she got back to her car she looked at the hanger and realized she didn't have a clue how to use the hanger to open the door.
Feeling quite hopeless, she bowed her head and asked God for help. Almost immediately an old rusty car pulled up, driven by a dirty, greasy, bearded man with a rag on his head.
The woman thought to herself, "Great. Is THIS what you sent to help me?" But she was desperate, and decided any help was better than no help at all.
The man got out of his car and asked if he could help.
"Yes, my daughter is very sick," the woman replied. "I must get home to her with this medicine, but I can't because I locked my keys in the car. Is there any way you can use this hanger to unlock my car?"
The man walked over to the car and in seconds the car was opened. Almost in tears, the woman expressed her appreciation.
"THANK YOU SO MUCH.....You are such a very nice man, and an answer to prayer!"
The man replied, "Lady, I ain't a nice man. I just got out of prison for car theft."
In even greater appreciation, the woman cried out loud, "THANK YOU FOR SENDING ME A PROFESSIONAL!"



simlpe and practical approach to acid base disturbance
systematic approach to interpretation of acid base ststus.
1. Examine arterial pH: Is acidemia or alkalemia present?
2. Examine PaCO2: Is the change in PaCO2 consistent with a respiratory component?
3. If the change in PaCO2 does not explain the change in arterial pH, does the change in [HCO3–] indicate a metabolic component?
4. Make a tentative diagnosis (see Tables below).
5. Compare the change in [HCO3–] with the change in PaCO2. Does a compensatory response exist? Because arterial pH is related to the ratio of PaCO2 to [HCO3–], both pulmonary and renal compensatory mechanisms are always such that PaCO2 and [HCO3–] change in the same direction. A change in opposite directions implies a mixed acid–base disorder.
6. If the compensatory response is more or less than expected, by definition a mixed acid–base disorder exists.
7. Calculate the plasma anion gap in the case of metabolic acidosis.
8. Measure urinary chloride concentration in the case of metabolic alkalosis.



Compensatory Mechanisms
Physiological responses to changes in [H+] are characterized by three phases: (1) immediate chemical buffering, (2) respiratory compensation (whenever possible), and (3) a slower but more effective renal compensatory response that may nearly normalize arterial pH even if the pathological process is still present.
immediate chemical buffur
bicarbonate buffur
hemoglobin buffur
intracellular proteins
phosphate and ammonia
the bicarbonate buffer consists of H2CO3 and HCO3–, CO2 tension (PCO2) may be substituted for H2CO3, because:
the Henderson–Hasselbalch equation for bicarbonate can be written as follows:
It should be emphasized that the bicarbonate buffer is effective against metabolic but not respiratory acid–base disturbances.
Changes in alveolar ventilation responsible for pulmonary compensation of PaCO2 are mediated by chemoreceptors within the brain stem in response to changes in cerebrospinal spinal fluid pH.
Pulmonary Compensation during Metabolic Acidosis
Decreases in arterial blood pH stimulate medullary respiratory centers. The resulting increase in alveolar ventilation lowers PaCO2 and tends to restore arterial pH toward normal.
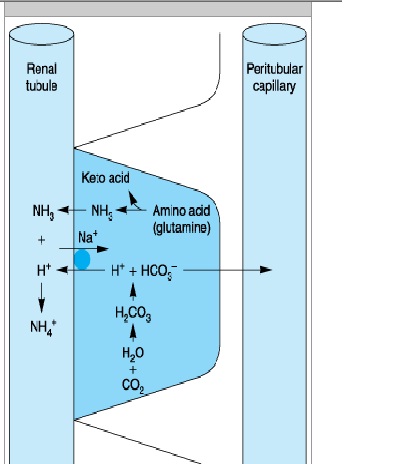
- control the amount of HCO3– reabsorbed from filtered tubular fluid
- form new HCO3–
- eliminate H+ in the form of titratable acids and ammonium ions
(1) increased reabsorption of the filtered HCO3–


(2) increased excretion of titratable acids


(3) increased production of ammonia.

Renal Compensation during Alkalosis
exceretion of large amount of HCO3.
Metabolic alkalosis is commonly associated with increased mineralocorticoid activity even in the absence of sodium and chloride depletion.
Base excess is the amount of acid or base that must be added for blood pH to return to 7.40 and PaCO2 to return to 40 mm Hg at full O2 saturation and 37°C.
Acidosis
· Direct myocardial and smooth muscle depression reduces cardiac contractility and peripheral vascular resistance, resulting in progressive hypotension.
· Progressive hyperkalemia as a result of the movement of K+ out of cells in exchange for extracellular H+ is also potentially lethal. Plasma [K+] increases approximately 0.6 mEq/L for each 0.10 decrease in pH.
· Central nervous system depression is more prominent with respiratory acidosis than with metabolic acidosis.
Respiratory acidosis is defined as a primary increase in PaCO2 leading to an increase in [H+] and a decrease in arterial pH.
Alveolar hypoventilation
· Central nervous system depression
· Neuromuscular disorders
· Chest wall abnormalities
· Pleural abnormalities
· Airway obstruction
· Parenchymal lung disease
· Ventilator malfunction
Increased CO2 production
· Large caloric loads
· Malignant hyperthermia
· Intensive shivering
· Prolonged seizure activity
· Thyroid storm
Acute Respiratory Acidosis
The compensatory response to acute (6–12 h) elevations in PaCO2 is limited. As a result, plasma [HCO3–] increases only about 1 mEq/L for each 10 mm Hg increase in PaCO2 above 40 mm Hg.
"Full" renal compensation characterizes chronic respiratory acidosis. plasma [HCO3–] increases approximately 4 mEq/L for each 10 mm Hg increase in PaCO2 above 40 mm Hg.
· Measures aimed at reducing CO2 production are useful only in specific instances (eg, dantrolene for malignant hyperthermia, muscle paralysis for tetanus, antithyroid medication for thyroid storm, and reduced caloric intake).
· Temporizing measures aimed at improving alveolar ventilation include bronchodilation, reversal of narcosis, administration of a respiratory stimulant (doxapram), or improving lung compliance (dieresis
· Intravenous NaHCO3 is rarely necessary unless pH is < 7.10 and HCO3– is < 15 mEq/L.
Patients with a baseline chronic respiratory acidosis require special consideration. When such patients develop acute ventilatory failure, the goal of therapy should be to return PaCO2 to the patient's "normal" baseline.
Metabolic Acidosis
Metabolic acidosis is defined as a primary decrease in [HCO3–]. Pathological processes can initiate metabolic acidosis by one of three mechanisms: (1) consumption of HCO3– by a strong nonvolatile acid, (2) renal or gastrointestinal wasting of bicarbonate, or (3) rapid dilution of the extracellular fluid compartment with a bicarbonate-free fluid.
Causes of Metabolic Acidosis.
Increased anion gap
Increased production of endogenous nonvolatile acids
· Renal failure
· Ketoacidosis
· Diabetic
· Starvation
· Lactic acidosis
· Mixed
· Nonketotic hyperosmolar coma
· Alcoholic
· Inborn errors of metabolism
· Ingestion of toxin:
o Salicylate
o Methanol
o Ethylene glycol
o Paraldehyde
o Toluene
o Sulfur
· Rhabdomyolysis
Normal anion gap (hyperchloremic)
Increased gastrointestinal losses of HCO3–
· Diarrhea
· Anion exchange resins (cholestyramine)
· Ingestion of CaCl2, MgCl2
· Fistulas (pancreatic, biliary, or small bowel)
· Ureterosigmoidostomy or obstructed ileal loop
Increased renal losses of HCO3–
· Renal tubular acidosis
· Carbonic anhydrase inhibitors
· Hypoaldosteronism
Dilutional
· Large amount of bicarbonate-free fluids
· Total parenteral nutrition (Cl– salts of amino acids)
Increased intake of chloride-containing acids
· Ammonium chloride
· Lysine hydrochloride
The Anion Gap
The anion gap in plasma is most commonly defined as the difference between the major measured cations and the major measured anions:
Anion Gap = 140 - _104 + 24) =12 mEq/L
Endogenously produced organic acids are normally eliminated by the kidneys in urine. Glomerular filtration rates below 20 mL/min (renal failure) typically result in progressive metabolic acidosis from the accumulation of these acids.
Severe tissue hypoxia following hypoxemia, hypoperfusion (ischemia), or inability to utilize oxygen (cyanide poisoning) can result in lactic acidosis.
Metabolic acidosis associated with a normal anion gap is typically characterized by hyperchloremia. Plasma [Cl–] increases to take the place of the HCO3– ions that are lost. Hyperchloremic metabolic acidosis most commonly results from abnormal gastrointestinal or renal losses of HCO3–.
Alkali therapy in the form of NaHCO3 is given if PH is below 7.20. the dose is decided empirically as a fixed dose (1 mEq/kg) or is derived from the base excess and the calculated bicarbonate space.
The bicarbonate space is defined as the volume to which HCO3– will distribute when it is given intravenously. Although this theoretically should equal the extracellular fluid space (approximately 25% of body weight), in reality it ranges anywhere between 25% and 60% of body weight depending on the severity and duration of the acidosis.
In practice, only 50% of the calculated dose (105 mEq) is usually given, after which another blood gas is measured.
· Acidemia can potentiate the depressant effects of most sedatives and anesthetic agents on the central nervous and circulatory systems. Increased sedation and depression of airway reflexes may predispose to pulmonary aspiration.
· Halothane is more arrhythmogenic in the presence of acidosis.
· Succinylcholine should generally be avoided in acidotic patients with hyperkalemia to prevent further increases in plasma [K+].
· Respiratory—but not metabolic—acidosis augments nondepolarizing neuromuscular blockade and may prevent its antagonism by reversal agents.
Alkalosis
· Alkalosis increases the affinity of hemoglobin for oxygen and shifts the oxygen dissociation curve to the left, making it more difficult for hemoglobin to give up oxygen to tissues.
· Movement of H+ out of cells in exchange for the movement of extracellular K+ into cells can produce hypokalemia.
· Alkalosis increases the number of anionic binding sites for Ca2+ on plasma proteins and can therefore decrease ionized plasma [Ca2+], leading to circulatory depression and neuromuscular irritability.
· Respiratory alkalosis reduces cerebral blood flow, increases systemic vascular resistance, and may precipitate coronary vasospasm.
· In the lungs, respiratory alkalosis increases bronchial smooth muscle tone (bronchoconstriction) but decreases pulmonary vascular resistance.
Causes of Respiratory Alkalosis.
Central stimulation
· Pain
· Anxiety
· Ischemia
· Stroke
· Tumor
· Infection
· Fever
· Drug-induced
· Salicylates
· Progesterone (pregnancy)
· Analeptics (doxapram)
Peripheral stimulation
· Hypoxemia
· High altitude
· Pulmonary disease
· Congestive heart failure
· Noncardiogenic pulmonary edema
· Asthma
· Pulmonary embolism
· Severe anemia
Unknown mechanism
Sepsis
Metabolic encephalopathies
Iatrogenic
Ventilator-induced
Treatment of Respiratory Alkalosis
Correction of the underlying process is the only treatment for respiratory alkalosis. For severe alkalemia (arterial pH > 7.60), intravenous hydrochloric acid, arginine chloride, or ammonium chloride may be indicated.
Metabolic alkalosis is defined as a primary increase in plasma [HCO3–]. Most cases of metabolic alkalosis can be divided into (1) those associated with NaCl deficiency and extracellular fluid depletion, often described as chloride sensitive, and (2) those associated with enhanced mineralocorticoid activity, commonly referred to as chloride resistant.
Chloride-sensitive
Gastrointestinal
· Vomiting
· Gastric drainage
Renal
· Diuretics
· Posthypercapnic
· Low chloride intake
Sweat
Cystic fibrosis
Chloride-resistant
· Increased mineralocorticoid activity
· Primary hyperaldosteronism
· Edematous disorders (secondary hyperaldosteronism)
· Cushing's syndrome
· Licorice ingestion
· Bartter's syndrome
· Severe hypokalemia
Miscellaneous
Massive blood transfusion
Acetate-containing colloid solutions
Alkaline administration with renal insufficiency
· The treatment of choice for chloride-sensitive metabolic alkalosis is administration of intravenous saline (NaCl) and potassium (KCl).
· Alkalosis associated with primary increases in mineralocorticoid activity readily responds to aldosterone antagonists (spironolactone).
· When arterial blood pH is greater than 7.60, treatment with intravenous hydrochloric acid (0.1 mol/L), ammonium chloride (0.1 mol/L), arginine hydrochloride, or hemodialysis should be considered.
· Cerebral ischemia can occur from marked reduction in cerebral blood flow during respiratory alkalosis, particularly during hypotension.
· The combination of alkalemia and hypokalemia can precipitate severe atrial and ventricular arrhythmias.
· Potentiation of nondepolarizing neuromuscular blockade is reported with alkalemia but may be more directly related to concomitant hypokalemia.
Subscribe to:
Comments (Atom)