systematic approach to interpretation of acid base ststus.
1. Examine arterial pH: Is acidemia or alkalemia present?
2. Examine PaCO2: Is the change in PaCO2 consistent with a respiratory component?
3. If the change in PaCO2 does not explain the change in arterial pH, does the change in [HCO3–] indicate a metabolic component?
4. Make a tentative diagnosis (see Tables below).
5. Compare the change in [HCO3–] with the change in PaCO2. Does a compensatory response exist? Because arterial pH is related to the ratio of PaCO2 to [HCO3–], both pulmonary and renal compensatory mechanisms are always such that PaCO2 and [HCO3–] change in the same direction. A change in opposite directions implies a mixed acid–base disorder.
6. If the compensatory response is more or less than expected, by definition a mixed acid–base disorder exists.
7. Calculate the plasma anion gap in the case of metabolic acidosis.
8. Measure urinary chloride concentration in the case of metabolic alkalosis.



Compensatory Mechanisms
Physiological responses to changes in [H+] are characterized by three phases: (1) immediate chemical buffering, (2) respiratory compensation (whenever possible), and (3) a slower but more effective renal compensatory response that may nearly normalize arterial pH even if the pathological process is still present.
immediate chemical buffur
bicarbonate buffur
hemoglobin buffur
intracellular proteins
phosphate and ammonia
the bicarbonate buffer consists of H2CO3 and HCO3–, CO2 tension (PCO2) may be substituted for H2CO3, because:
the Henderson–Hasselbalch equation for bicarbonate can be written as follows:
It should be emphasized that the bicarbonate buffer is effective against metabolic but not respiratory acid–base disturbances.
Changes in alveolar ventilation responsible for pulmonary compensation of PaCO2 are mediated by chemoreceptors within the brain stem in response to changes in cerebrospinal spinal fluid pH.
Pulmonary Compensation during Metabolic Acidosis
Decreases in arterial blood pH stimulate medullary respiratory centers. The resulting increase in alveolar ventilation lowers PaCO2 and tends to restore arterial pH toward normal.
- control the amount of HCO3– reabsorbed from filtered tubular fluid
- form new HCO3–
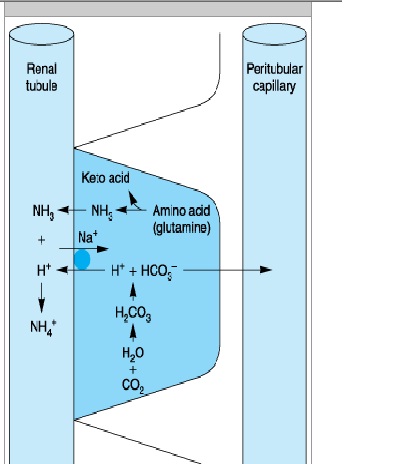
- eliminate H+ in the form of titratable acids and ammonium ions
(1) increased reabsorption of the filtered HCO3–


(2) increased excretion of titratable acids


(3) increased production of ammonia.

Renal Compensation during Alkalosis
exceretion of large amount of HCO3.
Metabolic alkalosis is commonly associated with increased mineralocorticoid activity even in the absence of sodium and chloride depletion.
Base excess is the amount of acid or base that must be added for blood pH to return to 7.40 and PaCO2 to return to 40 mm Hg at full O2 saturation and 37°C.
Acidosis
· Direct myocardial and smooth muscle depression reduces cardiac contractility and peripheral vascular resistance, resulting in progressive hypotension.
· Progressive hyperkalemia as a result of the movement of K+ out of cells in exchange for extracellular H+ is also potentially lethal. Plasma [K+] increases approximately 0.6 mEq/L for each 0.10 decrease in pH.
· Central nervous system depression is more prominent with respiratory acidosis than with metabolic acidosis.
Respiratory acidosis is defined as a primary increase in PaCO2 leading to an increase in [H+] and a decrease in arterial pH.
Alveolar hypoventilation
· Central nervous system depression
· Neuromuscular disorders
· Chest wall abnormalities
· Pleural abnormalities
· Airway obstruction
· Parenchymal lung disease
· Ventilator malfunction
Increased CO2 production
· Large caloric loads
· Malignant hyperthermia
· Intensive shivering
· Prolonged seizure activity
· Thyroid storm
Acute Respiratory Acidosis
The compensatory response to acute (6–12 h) elevations in PaCO2 is limited. As a result, plasma [HCO3–] increases only about 1 mEq/L for each 10 mm Hg increase in PaCO2 above 40 mm Hg.
"Full" renal compensation characterizes chronic respiratory acidosis. plasma [HCO3–] increases approximately 4 mEq/L for each 10 mm Hg increase in PaCO2 above 40 mm Hg.
· Measures aimed at reducing CO2 production are useful only in specific instances (eg, dantrolene for malignant hyperthermia, muscle paralysis for tetanus, antithyroid medication for thyroid storm, and reduced caloric intake).
· Temporizing measures aimed at improving alveolar ventilation include bronchodilation, reversal of narcosis, administration of a respiratory stimulant (doxapram), or improving lung compliance (dieresis
· Intravenous NaHCO3 is rarely necessary unless pH is < 7.10 and HCO3– is < 15 mEq/L.
Patients with a baseline chronic respiratory acidosis require special consideration. When such patients develop acute ventilatory failure, the goal of therapy should be to return PaCO2 to the patient's "normal" baseline.
Metabolic Acidosis
Metabolic acidosis is defined as a primary decrease in [HCO3–]. Pathological processes can initiate metabolic acidosis by one of three mechanisms: (1) consumption of HCO3– by a strong nonvolatile acid, (2) renal or gastrointestinal wasting of bicarbonate, or (3) rapid dilution of the extracellular fluid compartment with a bicarbonate-free fluid.
Causes of Metabolic Acidosis.
Increased anion gap
Increased production of endogenous nonvolatile acids
· Renal failure
· Ketoacidosis
· Diabetic
· Starvation
· Lactic acidosis
· Mixed
· Nonketotic hyperosmolar coma
· Alcoholic
· Inborn errors of metabolism
· Ingestion of toxin:
o Salicylate
o Methanol
o Ethylene glycol
o Paraldehyde
o Toluene
o Sulfur
· Rhabdomyolysis
Normal anion gap (hyperchloremic)
Increased gastrointestinal losses of HCO3–
· Diarrhea
· Anion exchange resins (cholestyramine)
· Ingestion of CaCl2, MgCl2
· Fistulas (pancreatic, biliary, or small bowel)
· Ureterosigmoidostomy or obstructed ileal loop
Increased renal losses of HCO3–
· Renal tubular acidosis
· Carbonic anhydrase inhibitors
· Hypoaldosteronism
Dilutional
· Large amount of bicarbonate-free fluids
· Total parenteral nutrition (Cl– salts of amino acids)
Increased intake of chloride-containing acids
· Ammonium chloride
· Lysine hydrochloride
The Anion Gap
The anion gap in plasma is most commonly defined as the difference between the major measured cations and the major measured anions:
Anion Gap = 140 - _104 + 24) =12 mEq/L
Endogenously produced organic acids are normally eliminated by the kidneys in urine. Glomerular filtration rates below 20 mL/min (renal failure) typically result in progressive metabolic acidosis from the accumulation of these acids.
Severe tissue hypoxia following hypoxemia, hypoperfusion (ischemia), or inability to utilize oxygen (cyanide poisoning) can result in lactic acidosis.
Metabolic acidosis associated with a normal anion gap is typically characterized by hyperchloremia. Plasma [Cl–] increases to take the place of the HCO3– ions that are lost. Hyperchloremic metabolic acidosis most commonly results from abnormal gastrointestinal or renal losses of HCO3–.
Alkali therapy in the form of NaHCO3 is given if PH is below 7.20. the dose is decided empirically as a fixed dose (1 mEq/kg) or is derived from the base excess and the calculated bicarbonate space.
The bicarbonate space is defined as the volume to which HCO3– will distribute when it is given intravenously. Although this theoretically should equal the extracellular fluid space (approximately 25% of body weight), in reality it ranges anywhere between 25% and 60% of body weight depending on the severity and duration of the acidosis.
In practice, only 50% of the calculated dose (105 mEq) is usually given, after which another blood gas is measured.
· Acidemia can potentiate the depressant effects of most sedatives and anesthetic agents on the central nervous and circulatory systems. Increased sedation and depression of airway reflexes may predispose to pulmonary aspiration.
· Halothane is more arrhythmogenic in the presence of acidosis.
· Succinylcholine should generally be avoided in acidotic patients with hyperkalemia to prevent further increases in plasma [K+].
· Respiratory—but not metabolic—acidosis augments nondepolarizing neuromuscular blockade and may prevent its antagonism by reversal agents.
Alkalosis
· Alkalosis increases the affinity of hemoglobin for oxygen and shifts the oxygen dissociation curve to the left, making it more difficult for hemoglobin to give up oxygen to tissues.
· Movement of H+ out of cells in exchange for the movement of extracellular K+ into cells can produce hypokalemia.
· Alkalosis increases the number of anionic binding sites for Ca2+ on plasma proteins and can therefore decrease ionized plasma [Ca2+], leading to circulatory depression and neuromuscular irritability.
· Respiratory alkalosis reduces cerebral blood flow, increases systemic vascular resistance, and may precipitate coronary vasospasm.
· In the lungs, respiratory alkalosis increases bronchial smooth muscle tone (bronchoconstriction) but decreases pulmonary vascular resistance.
Causes of Respiratory Alkalosis.
Central stimulation
· Pain
· Anxiety
· Ischemia
· Stroke
· Tumor
· Infection
· Fever
· Drug-induced
· Salicylates
· Progesterone (pregnancy)
· Analeptics (doxapram)
Peripheral stimulation
· Hypoxemia
· High altitude
· Pulmonary disease
· Congestive heart failure
· Noncardiogenic pulmonary edema
· Asthma
· Pulmonary embolism
· Severe anemia
Unknown mechanism
Sepsis
Metabolic encephalopathies
Iatrogenic
Ventilator-induced
Treatment of Respiratory Alkalosis
Correction of the underlying process is the only treatment for respiratory alkalosis. For severe alkalemia (arterial pH > 7.60), intravenous hydrochloric acid, arginine chloride, or ammonium chloride may be indicated.
Metabolic alkalosis is defined as a primary increase in plasma [HCO3–]. Most cases of metabolic alkalosis can be divided into (1) those associated with NaCl deficiency and extracellular fluid depletion, often described as chloride sensitive, and (2) those associated with enhanced mineralocorticoid activity, commonly referred to as chloride resistant.
Chloride-sensitive
Gastrointestinal
· Vomiting
· Gastric drainage
Renal
· Diuretics
· Posthypercapnic
· Low chloride intake
Sweat
Cystic fibrosis
Chloride-resistant
· Increased mineralocorticoid activity
· Primary hyperaldosteronism
· Edematous disorders (secondary hyperaldosteronism)
· Cushing's syndrome
· Licorice ingestion
· Bartter's syndrome
· Severe hypokalemia
Miscellaneous
Massive blood transfusion
Acetate-containing colloid solutions
Alkaline administration with renal insufficiency
· The treatment of choice for chloride-sensitive metabolic alkalosis is administration of intravenous saline (NaCl) and potassium (KCl).
· Alkalosis associated with primary increases in mineralocorticoid activity readily responds to aldosterone antagonists (spironolactone).
· When arterial blood pH is greater than 7.60, treatment with intravenous hydrochloric acid (0.1 mol/L), ammonium chloride (0.1 mol/L), arginine hydrochloride, or hemodialysis should be considered.
· Cerebral ischemia can occur from marked reduction in cerebral blood flow during respiratory alkalosis, particularly during hypotension.
· The combination of alkalemia and hypokalemia can precipitate severe atrial and ventricular arrhythmias.
· Potentiation of nondepolarizing neuromuscular blockade is reported with alkalemia but may be more directly related to concomitant hypokalemia.
Really good explanation. This is informative for me. Thanks for giving acknowledgment such like this.
ReplyDeletethanks! ive been looking for these for my assignment..thank you so much!
ReplyDeleteMay ӏ simply just say ωhаt a comfort to diѕcovеr someone who genuinеly underѕtands what theу're talking about on the net. You certainly understand how to bring a problem to light and make it important. More and more people should read this and understand this side of the story. I was surprised that you're not mоre popular because you suгely have the gіft.
ReplyDeleteAlso see my site :: symptoms of kidney cancer
nice !!!
ReplyDelete